Over-Pronation Of The Foot What Are The Treatments
Overview
The rolling of the foot is a natural process and the degree to which pronation occurs will depend on an individual?s gait. It has been suggested that up to 70 percent of runners may overpronate to some degree, although it is not always bad for the body even though pronation may not be at optimum levels. Slight overpronation may be perfectly acceptable and may not place an individual at an increased risk of injury; however determining whether this is the case can only come from a doctor, podiatrist or sports therapist. While specialist running shoe stores may be able to spot whether you are an overpronator after observing you on a treadmill and suggest the best running shoes to suit your gait, it is still wise if you are an overpronator to get your gait checked professionally.
Causes
Congenital "Flat Feet" - an individual may be born with feet that lack an appropriately supportive arch thereby predisposing the individual to this foot condition. Excessive Weight (Obesity) Too much weight on the foot from either obesity or pregnancy may be a factor. Repetitive Impact walking on flat, hard surfaces continuously places unnatural stress on the foot arch.
Symptoms
Common conditions seen with overpronation include heel pain or plantar fasciitis. Achilles tendonopathy. Hallus Valgus and/or bunions. Patellofemoral pain syndrome. Iliotibial band pain syndrome. Low back pain. Shin splints. Stress fractures in the foot or lower leg.
Diagnosis
At some point you may find the pain to much or become frustrated. So what are you options? Chances are your overpronation has led to some type of injury if there's pain. Your best bet is to consult with someone who knows feet. Start with your pediatrist, chiropodist or chiropractor. They'll be able to diagnose and treat the injury and give you more specific direction to better support your feet. One common intervention is a custom foot orthotic. Giving greater structural support than a typical shoe these shoe inserts can dramatically reduce overpronation.
Non Surgical Treatment
Overpronation is a condition in which the foot rolls excessively down and inward. The arch may elongate and collapse (or ?fall?) and the heel will lean inward. Overpronation should not be confused with pronation. Pronation is a normal motion of the foot during weight bearing and allows the foot to absorb shock as it contacts the ground.
Prevention
Many of the prevention methods for overpronation orthotics, for example, can be used interchangeably with treatment methods. If the overpronation is severe, you should seek medical attention from a podiatrist who can cast you for custom-made orthotics. Custom-made orthotics are more expensive, but they last longer and provide support, stability, and balance for the entire foot. You can also talk with a shoe specialist about running shoes that offer extra medial support and firm heel counters. Proper shoes can improve symptoms quickly and prevent them from recurring. Surgery can sometimes help cure and prevent this problem if you suffer from inherited or acquired pes planus deformity. Surgery typically involves stabilizing the bones to improve the foot?s support and function.
The rolling of the foot is a natural process and the degree to which pronation occurs will depend on an individual?s gait. It has been suggested that up to 70 percent of runners may overpronate to some degree, although it is not always bad for the body even though pronation may not be at optimum levels. Slight overpronation may be perfectly acceptable and may not place an individual at an increased risk of injury; however determining whether this is the case can only come from a doctor, podiatrist or sports therapist. While specialist running shoe stores may be able to spot whether you are an overpronator after observing you on a treadmill and suggest the best running shoes to suit your gait, it is still wise if you are an overpronator to get your gait checked professionally.
Causes
Congenital "Flat Feet" - an individual may be born with feet that lack an appropriately supportive arch thereby predisposing the individual to this foot condition. Excessive Weight (Obesity) Too much weight on the foot from either obesity or pregnancy may be a factor. Repetitive Impact walking on flat, hard surfaces continuously places unnatural stress on the foot arch.
Symptoms
Common conditions seen with overpronation include heel pain or plantar fasciitis. Achilles tendonopathy. Hallus Valgus and/or bunions. Patellofemoral pain syndrome. Iliotibial band pain syndrome. Low back pain. Shin splints. Stress fractures in the foot or lower leg.
Diagnosis
At some point you may find the pain to much or become frustrated. So what are you options? Chances are your overpronation has led to some type of injury if there's pain. Your best bet is to consult with someone who knows feet. Start with your pediatrist, chiropodist or chiropractor. They'll be able to diagnose and treat the injury and give you more specific direction to better support your feet. One common intervention is a custom foot orthotic. Giving greater structural support than a typical shoe these shoe inserts can dramatically reduce overpronation.
Non Surgical Treatment
Overpronation is a condition in which the foot rolls excessively down and inward. The arch may elongate and collapse (or ?fall?) and the heel will lean inward. Overpronation should not be confused with pronation. Pronation is a normal motion of the foot during weight bearing and allows the foot to absorb shock as it contacts the ground.
Prevention
Many of the prevention methods for overpronation orthotics, for example, can be used interchangeably with treatment methods. If the overpronation is severe, you should seek medical attention from a podiatrist who can cast you for custom-made orthotics. Custom-made orthotics are more expensive, but they last longer and provide support, stability, and balance for the entire foot. You can also talk with a shoe specialist about running shoes that offer extra medial support and firm heel counters. Proper shoes can improve symptoms quickly and prevent them from recurring. Surgery can sometimes help cure and prevent this problem if you suffer from inherited or acquired pes planus deformity. Surgery typically involves stabilizing the bones to improve the foot?s support and function.
Calcaneal Apophysitis Rehab
Overview
The calcaneal apophysis is a growth center where the Achilles tendon and the plantar fascia attach to the heel. It first appears in children aged 7 to 8 years. By ages 12 to 14 years the growth center matures and fuses to the heel bone. Injuries can occur from excessive tension on the Achilles tendon and the plantar fascia, or from direct impact on the heel. Excessive stress on this growth center can cause irritation of the heel, also called Sever?s disease.
Causes
Sever condition is caused by sprain injury where the Achilles tendon attaches to the calcaneus bone at the back of the heel. Sever condition occurs in adolescent or older children, particularly active boys. It can be very painful. It is one of those conditions commonly referred to as "growing pains." Patients are evaluated for signs of conditions that can mimic Sever condition, such as ankylosing spondylitis and other forms of arthritis. Usually Sever condition is self-limited; that is, it disappears as the child ages.
Symptoms
The main symptom of sever's disease is pain and tenderness at the back of the heel which is made worse with physical activity. Tenderness will be felt especially if you press in or give the back of the heel a squeeze from the sides. There may be a lump over the painful area. Another sign is tight calf muscles resulting with reduced range of motion at the ankle. Pain may go away after a period of rest from sporting activities only to return when the young person goes back to training.
Diagnosis
You may have pain when your doctor squeezes your heel bone. You may have pain when asked to stand or walk on your toes or on your heels. You may have pain in your heel when your doctor stretches your calf muscles. Your doctor may order x-rays of the injured foot to show an active growth plate.
Non Surgical Treatment
Your child may need to change or stop doing the activities that cause pain until the growth plate heals. Your child needs to wear shoes with good padding in the heels and good arch support. Special shoes or shoe inserts may help. Pain from Sever's disease may last weeks to months. The pain may come back if your child returns to sports or strenuous activities too soon.
Prevention
Because there are several theories as to the actual cause of the disease, there is no definitive answer on prevention. Experts agree, though, that youth athletes can help minimize the risk of Sever's disease by maintaining good joint and muscle flexibility while engaging in sports or physical activities.
The calcaneal apophysis is a growth center where the Achilles tendon and the plantar fascia attach to the heel. It first appears in children aged 7 to 8 years. By ages 12 to 14 years the growth center matures and fuses to the heel bone. Injuries can occur from excessive tension on the Achilles tendon and the plantar fascia, or from direct impact on the heel. Excessive stress on this growth center can cause irritation of the heel, also called Sever?s disease.
Causes
Sever condition is caused by sprain injury where the Achilles tendon attaches to the calcaneus bone at the back of the heel. Sever condition occurs in adolescent or older children, particularly active boys. It can be very painful. It is one of those conditions commonly referred to as "growing pains." Patients are evaluated for signs of conditions that can mimic Sever condition, such as ankylosing spondylitis and other forms of arthritis. Usually Sever condition is self-limited; that is, it disappears as the child ages.
Symptoms
The main symptom of sever's disease is pain and tenderness at the back of the heel which is made worse with physical activity. Tenderness will be felt especially if you press in or give the back of the heel a squeeze from the sides. There may be a lump over the painful area. Another sign is tight calf muscles resulting with reduced range of motion at the ankle. Pain may go away after a period of rest from sporting activities only to return when the young person goes back to training.
Diagnosis
You may have pain when your doctor squeezes your heel bone. You may have pain when asked to stand or walk on your toes or on your heels. You may have pain in your heel when your doctor stretches your calf muscles. Your doctor may order x-rays of the injured foot to show an active growth plate.
Non Surgical Treatment
Your child may need to change or stop doing the activities that cause pain until the growth plate heals. Your child needs to wear shoes with good padding in the heels and good arch support. Special shoes or shoe inserts may help. Pain from Sever's disease may last weeks to months. The pain may come back if your child returns to sports or strenuous activities too soon.
Prevention
Because there are several theories as to the actual cause of the disease, there is no definitive answer on prevention. Experts agree, though, that youth athletes can help minimize the risk of Sever's disease by maintaining good joint and muscle flexibility while engaging in sports or physical activities.
Treating Flat Feet In Adults
Overview
The posterior tibial tendon serves as one of the major supporting structures of the foot, helping it to function while walking. Posterior tibial tendon dysfunction (PTTD) is a condition caused by changes in the tendon, impairing its ability to support the arch. This results in flattening of the foot. PTTD is often called ?adult acquired flatfoot? because it is the most common type of flatfoot developed during adulthood. Although this condition typically occurs in only one foot, some people may develop it in both feet. PTTD is usually progressive, which means it will keep getting worse, especially if it isn?t treated early. 
Causes
The cause of posterior tibial tendon insufficiency is not completely understood. The condition commonly does not start from one acute trauma but is a process of gradual degeneration of the soft tissues supporting the medial (inner) side of the foot. It is most often associated with a foot that started out somewhat flat or pronated (rolled inward). This type of foot places more stress on the medial soft tissue structures, which include the posterior tibial tendon and ligaments on the inner side of the foot. Children nearly fully grown can end up with flat feet, the majority of which are no problem. However, if the deformity is severe enough it can cause significant functional limitations at that age and later on if soft tissue failure occurs. Also, young adults with normally aligned feet can acutely injure their posterior tibial tendon from a trauma and not develop deformity. The degenerative condition in patients beyond their twenties is different from the acute injuries in young patients or adolescent deformities, where progression of deformity is likely to occur.
Symptoms
The symptoms of PTTD may include pain, swelling, a flattening of the arch, and an inward rolling of the ankle. As the condition progresses, the symptoms will change. For example, when PTTD initially develops, there is pain on the inside of the foot and ankle (along the course of the tendon). In addition, the area may be red, warm, and swollen. Later, as the arch begins to flatten, there may still be pain on the inside of the foot and ankle. But at this point, the foot and toes begin to turn outward and the ankle rolls inward. As PTTD becomes more advanced, the arch flattens even more and the pain often shifts to the outside of the foot, below the ankle. The tendon has deteriorated considerably and arthritis often develops in the foot. In more severe cases, arthritis may also develop in the ankle.
Diagnosis
The history and physical examination are probably the most important tools the physician uses to diagnose this problem. The wear pattern on your shoes can offer some helpful clues. Muscle testing helps identify any areas of weakness or muscle impairment. This should be done in both the weight bearing and nonweight bearing positions. A very effective test is the single heel raise. You will be asked to stand on one foot and rise up on your toes. You should be able to lift your heel off the ground easily while keeping the calcaneus (heel bone) in the middle with slight inversion (turned inward). X-rays are often used to study the position, shape, and alignment of the bones in the feet and ankles. Magnetic resonance (MR) imaging is the imaging modality of choice for evaluating the posterior tibial tendon and spring ligament complex.
Non surgical Treatment
Stage one deformities usually respond to conservative or non-surgical therapy such as anti-inflammatory medication, casting, functional orthotics or a foot ankle orthosis called a Richie Brace. If these modalities are unsuccessful surgery is warranted. 
Surgical Treatment
Surgery is usually performed when non-surgical measures have failed. The goal of surgery is to eliminate pain, stop progression of the deformity and improve a patient?s mobility. More than one technique may be used, and surgery tends to include one or more of the following. The tendon is reconstructed or replaced using another tendon in the foot or ankle The name of the technique depends on the tendon used. Flexor digitorum longus (FDL) transfer. Flexor hallucis longus (FHL) transfer. Tibialis anterior transfer (Cobb procedure). Calcaneal osteotomy - the heel bone may be shifted to bring your heel back under your leg and the position fixed with a screw. Lengthening of the Achilles tendon if it is particularly tight. Repair one of the ligaments under your foot. If you smoke, your surgeon may refuse to operate unless you can refrain from smoking before and during the healing phase of your procedure. Research has proven that smoking delays bone healing significantly.
Will Adult Aquired FlatFeet Necessitate Surgical Teatment ?
Overview
Often considered solely a product of genetics, flatfoot rarely carries with it the stigma of presenting over time. The truth, however, is that flatfoot does not discriminate on the basis of age and can become an issue in the form of adult-acquired flatfoot. Like its congenital cousin, adult-acquired flatfoot deformity is one that, in causing structural damage to the foot (and particularly to the posterior tibial tendon), creates an imbalance that may result in any number of symptoms, including inflammation, pain, stiffness, limited mobility, and even arthritis.
Causes
Women are affected by Adult Acquired Flatfoot four times more frequently than men. Adult Flatfoot generally occurs in middle to older age people. Most people who acquire the condition already have flat feet. One arch begins to flatten more, then pain and swelling develop on the inside of the ankle. This condition generally affects only one foot. It is unclear why women are affected more often than men. But factors that may increase your risk of Adult Flatfoot include diabetes, hypertension, and obesity.
Symptoms
The symptoms of PTTD may include pain, swelling, a flattening of the arch, and an inward rolling of the ankle. As the condition progresses, the symptoms will change. For example, when PTTD initially develops, there is pain on the inside of the foot and ankle (along the course of the tendon). In addition, the area may be red, warm, and swollen. Later, as the arch begins to flatten, there may still be pain on the inside of the foot and ankle. But at this point, the foot and toes begin to turn outward and the ankle rolls inward. As PTTD becomes more advanced, the arch flattens even more and the pain often shifts to the outside of the foot, below the ankle. The tendon has deteriorated considerably and arthritis often develops in the foot. In more severe cases, arthritis may also develop in the ankle.
Diagnosis
Posterior Tibial Tendon Dysfunction is diagnosed with careful clinical observation of the patient?s gait (walking), range of motion testing for the foot and ankle joints, and diagnostic imaging. People with flatfoot deformity walk with the heel angled outward, also called over-pronation. Although it is normal for the arch to impact the ground for shock absorption, people with PTTD have an arch that fully collapses to the ground and does not reform an arch during the entire gait period. After evaluating the ambulation pattern, the foot and ankle range of motion should be tested. Usually the affected foot will have decreased motion to the ankle joint and the hindfoot. Muscle strength may also be weaker as well. An easy test to perform for PTTD is the single heel raise where the patient is asked to raise up on the ball of his or her effected foot. A normal foot type can lift up on the toes without pain and the heel will invert slightly once the person has fully raised the heel up during the test. In early phases of PTTD the patient may be able to lift up the heel but the heel will not invert. An elongated or torn posterior tibial tendon, which is a mid to late finding of PTTD, will prohibit the patient from fully rising up on the heel and will cause intense pain to the arch. Finally diagnostic imaging, although used alone cannot diagnose PTTD, can provide additional information for an accurate diagnosis of flatfoot deformity. Xrays of the foot can show the practitioner important angular relationships of the hindfoot and forefoot which help diagnose flatfoot deformity. Most of the time, an MRI is not needed to diagnose PTTD but is a tool that should be considered in advanced cases of flatfoot deformity. If a partial tear of the posterior tibial tendon is of concern, then an MRI can show the anatomic location of the tear and the extensiveness of the injury.
Non surgical Treatment
Flatfoot can be treated with a variety of methods, including modified shoes, orthotic devices, a brace or cast, anti-inflammatory medications or limited steroid injections, rest, ice, and physical therapy. In severe cases, surgery may be necessary.

Surgical Treatment
Flatfoot reconstruction (osteotomy). This is often recommended for flexible flatfoot condition. Flatfoot reconstruction involves cutting and shifting the heel bone into a more neutral position, transferring the tendon used to flex the lesser toes (all but the big toe) to strengthen the posterior tibial tendon, and lengthening the calf muscle. Fusion (also known as triple arthrodesis). Fusion involves fusing, or making stiff, three joints in the back of the foot the subtalar, talonavicular, and calcaneocuboid joints, to realign the foot and give it a more natural shape. Pins or screws hold the area in place until it heals. Fusion is often recommended for a rigid flatfoot deformity or evidence of arthritis. Both of these surgeries can provide excellent pain relief and correction.
Often considered solely a product of genetics, flatfoot rarely carries with it the stigma of presenting over time. The truth, however, is that flatfoot does not discriminate on the basis of age and can become an issue in the form of adult-acquired flatfoot. Like its congenital cousin, adult-acquired flatfoot deformity is one that, in causing structural damage to the foot (and particularly to the posterior tibial tendon), creates an imbalance that may result in any number of symptoms, including inflammation, pain, stiffness, limited mobility, and even arthritis.
Causes
Women are affected by Adult Acquired Flatfoot four times more frequently than men. Adult Flatfoot generally occurs in middle to older age people. Most people who acquire the condition already have flat feet. One arch begins to flatten more, then pain and swelling develop on the inside of the ankle. This condition generally affects only one foot. It is unclear why women are affected more often than men. But factors that may increase your risk of Adult Flatfoot include diabetes, hypertension, and obesity.
Symptoms
The symptoms of PTTD may include pain, swelling, a flattening of the arch, and an inward rolling of the ankle. As the condition progresses, the symptoms will change. For example, when PTTD initially develops, there is pain on the inside of the foot and ankle (along the course of the tendon). In addition, the area may be red, warm, and swollen. Later, as the arch begins to flatten, there may still be pain on the inside of the foot and ankle. But at this point, the foot and toes begin to turn outward and the ankle rolls inward. As PTTD becomes more advanced, the arch flattens even more and the pain often shifts to the outside of the foot, below the ankle. The tendon has deteriorated considerably and arthritis often develops in the foot. In more severe cases, arthritis may also develop in the ankle.
Diagnosis
Posterior Tibial Tendon Dysfunction is diagnosed with careful clinical observation of the patient?s gait (walking), range of motion testing for the foot and ankle joints, and diagnostic imaging. People with flatfoot deformity walk with the heel angled outward, also called over-pronation. Although it is normal for the arch to impact the ground for shock absorption, people with PTTD have an arch that fully collapses to the ground and does not reform an arch during the entire gait period. After evaluating the ambulation pattern, the foot and ankle range of motion should be tested. Usually the affected foot will have decreased motion to the ankle joint and the hindfoot. Muscle strength may also be weaker as well. An easy test to perform for PTTD is the single heel raise where the patient is asked to raise up on the ball of his or her effected foot. A normal foot type can lift up on the toes without pain and the heel will invert slightly once the person has fully raised the heel up during the test. In early phases of PTTD the patient may be able to lift up the heel but the heel will not invert. An elongated or torn posterior tibial tendon, which is a mid to late finding of PTTD, will prohibit the patient from fully rising up on the heel and will cause intense pain to the arch. Finally diagnostic imaging, although used alone cannot diagnose PTTD, can provide additional information for an accurate diagnosis of flatfoot deformity. Xrays of the foot can show the practitioner important angular relationships of the hindfoot and forefoot which help diagnose flatfoot deformity. Most of the time, an MRI is not needed to diagnose PTTD but is a tool that should be considered in advanced cases of flatfoot deformity. If a partial tear of the posterior tibial tendon is of concern, then an MRI can show the anatomic location of the tear and the extensiveness of the injury.
Non surgical Treatment
Flatfoot can be treated with a variety of methods, including modified shoes, orthotic devices, a brace or cast, anti-inflammatory medications or limited steroid injections, rest, ice, and physical therapy. In severe cases, surgery may be necessary.
Surgical Treatment
Flatfoot reconstruction (osteotomy). This is often recommended for flexible flatfoot condition. Flatfoot reconstruction involves cutting and shifting the heel bone into a more neutral position, transferring the tendon used to flex the lesser toes (all but the big toe) to strengthen the posterior tibial tendon, and lengthening the calf muscle. Fusion (also known as triple arthrodesis). Fusion involves fusing, or making stiff, three joints in the back of the foot the subtalar, talonavicular, and calcaneocuboid joints, to realign the foot and give it a more natural shape. Pins or screws hold the area in place until it heals. Fusion is often recommended for a rigid flatfoot deformity or evidence of arthritis. Both of these surgeries can provide excellent pain relief and correction.
What Is The Leading Cause Of Achilles Tendinitis ?
Overview
 The Achilles tendon is the largest tendon in the body. It connects the calf muscles to the heel and is active during almost all activities including walking, jumping, and swimming. This dense tendon can withstand large forces, but can become inflamed and painful during periods of overuse. Pain results from inflammation (tendonitis) or a degenerating tendon (tendinosis). Achilles tendon pathologies include rupture and tendonitis. Many experts now believe, however, that tendonitis is a misleading term that should no longer be used, because signs of true inflammation are almost never present on histologic examination. Instead, the following histopathologically determined nomenclature has evolved. Paratenonitis: Characterized by paratenon inflammation and thickening, as well as fibrin adhesions. Tendinosis: Characterized by intrasubstance disarray and degeneration of the tendon.
The Achilles tendon is the largest tendon in the body. It connects the calf muscles to the heel and is active during almost all activities including walking, jumping, and swimming. This dense tendon can withstand large forces, but can become inflamed and painful during periods of overuse. Pain results from inflammation (tendonitis) or a degenerating tendon (tendinosis). Achilles tendon pathologies include rupture and tendonitis. Many experts now believe, however, that tendonitis is a misleading term that should no longer be used, because signs of true inflammation are almost never present on histologic examination. Instead, the following histopathologically determined nomenclature has evolved. Paratenonitis: Characterized by paratenon inflammation and thickening, as well as fibrin adhesions. Tendinosis: Characterized by intrasubstance disarray and degeneration of the tendon.
Causes
The majority of Achilles tendon injuries are due to overuse injuries. Other factors that lead to Achilles tendonitis are improper shoe selection, inadequate stretching prior to engaging in athletics, a short Achilles tendon, direct trauma (injury) to the tendon, training errors and heel bone deformity. There is significant evidence that people with feet that role in excessively (over-pronate) are at greater risk for developing Achilles tendinitis. The increased pronation puts additional stress on the tendon, therefore, placing it at greater risk for injury.
Symptoms
The symptoms associated with Achilles tendonitis and tendonosis include, Pain-aching, stiffness, soreness, or tenderness-within the tendon. This may occur anywhere along the tendon?s path, beginning with the tendon?s attachment directly above the heel upward to the region just below the calf muscle. Often pain appears upon arising in the morning or after periods of rest, then improves somewhat with motion but later worsens with increased activity. Tenderness, or sometimes intense pain, when the sides of the tendon are squeezed. There is less tenderness, however, when pressing directly on the back of the tendon. When the disorder progresses to degeneration, the tendon may become enlarged and may develop nodules in the area where the tissue is damaged.
Diagnosis
Examination of the achilles tendon is inspection for muscle atrophy, swelling, asymmetry, joint effusions and erythema. Atrophy is an important clue to the duration of the tendinopathy and it is often present with chronic conditions. Swelling, asymmetry and erythema in pathologic tendons are often observed in the examination. Joint effusions are uncommon with tendinopathy and suggest the possibility of intra-articular pathology. Range of motion testing, strength and flexibility are often limited on the side of the tendinopathy. Palpation tends to elicit well-localized tenderness that is similar in quality and location to the pain experienced during activity. Physical examinations of the Achilles tendon often reveals palpable nodules and thickening. Anatomic deformities, such as forefoot and heel varus and excessive pes planus or foot pronation, should receive special attention. These anatomic deformities are often associated with this problem. In case extra research is wanted, an echography is the first choice of examination when there is a suspicion of tendinosis. Imaging studies are not necessary to diagnose achilles tendonitis, but may be useful with differential diagnosis. Ultrasound is the imaging modality of first choice as it provides a clear indication of tendon width, changes of water content within the tendon and collagen integrity, as well as bursal swelling. MRI may be indicated if diagnosis is unclear or symptoms are atypical. MRI may show increased signal within the Achilles.
Nonsurgical Treatment
There is insufficient evidence from randomised controlled trials to determine which method of treatment is the most appropriate for the treatment of acute or chronic Achilles tendonitis. The patient should abstain from aggravating activities, but with a minimum of rest in order to preserve overall fitness. Possible treatments are non-steroidal anti-inflammatory drugs (NSAIDs), ice, rest, increased warm-up/stretching exercises, physiotherapy and heel lifts (orthotic devices - used on both sides to prevent a gait imbalance). Other treatments evaluated in a Cochrane review were heparin, steroid injections, glycosaminoglycan sulfate, Actovegin?, and topical laser treatment. There was no clear evidence of benefit from these. Casting is an option for resistant Achilles tendonitis. Drugs - analgesics and NSAIDs. Surgery is sometimes used for resistant Achilles tendonitis, but usually as a last resort. Other recently reported treatments include continuing sporting activity in conjunction with rehabilitation, low-energy shock wave therapy[4] and topical glyceryl trinitrate .

Surgical Treatment
Surgery is considered when non-operative measures fail. Patient compliance and postoperative management is an important aspect of the operative management to prevent ankle stiffness or recurrence of the symptoms. Surgery usually requires a removal of the damaged tissue (debridement) and meticulous repair of the tendon. Post-operative immobilization is required, followed by gradual range of motion and strengthening exercises start. It may require 6 months for the full recovery. Some known complication are recurrence, stiffness of the ankle and deep vein thrombosis.
Prevention
Regardless of whether the Achilles injury is insertional or non-insertional, a great method for lessening stress on the Achilles tendon is flexor digitorum longus exercises. This muscle, which originates along the back of the leg and attaches to the tips of the toes, lies deep to the Achilles. It works synergistically with the soleus muscle to decelerate the forward motion of the leg before the heel leaves the ground during propulsion. This significantly lessens strain on the Achilles tendon as it decelerates elongation of the tendon. Many foot surgeons are aware of the connection between flexor digitorum longus and the Achilles tendon-surgical lengthening of the Achilles (which is done to treat certain congenital problems) almost always results in developing hammer toes as flexor digitorum longus attempts to do the job of the recently lengthened tendon. Finally, avoid having cortisone injected into either the bursa or tendon-doing so weakens the tendon as it shifts production of collagen from type one to type three. In a recent study published in the Journal of Bone Joint Surgery(9), cortisone was shown to lower the stress necessary to rupture the Achilles tendon, and was particularly dangerous when done on both sides, as it produced a systemic effect that further weakened the tendon.
The Achilles tendon is the largest tendon in the body. It connects the calf muscles to the heel and is active during almost all activities including walking, jumping, and swimming. This dense tendon can withstand large forces, but can become inflamed and painful during periods of overuse. Pain results from inflammation (tendonitis) or a degenerating tendon (tendinosis). Achilles tendon pathologies include rupture and tendonitis. Many experts now believe, however, that tendonitis is a misleading term that should no longer be used, because signs of true inflammation are almost never present on histologic examination. Instead, the following histopathologically determined nomenclature has evolved. Paratenonitis: Characterized by paratenon inflammation and thickening, as well as fibrin adhesions. Tendinosis: Characterized by intrasubstance disarray and degeneration of the tendon.
Causes
The majority of Achilles tendon injuries are due to overuse injuries. Other factors that lead to Achilles tendonitis are improper shoe selection, inadequate stretching prior to engaging in athletics, a short Achilles tendon, direct trauma (injury) to the tendon, training errors and heel bone deformity. There is significant evidence that people with feet that role in excessively (over-pronate) are at greater risk for developing Achilles tendinitis. The increased pronation puts additional stress on the tendon, therefore, placing it at greater risk for injury.
Symptoms
The symptoms associated with Achilles tendonitis and tendonosis include, Pain-aching, stiffness, soreness, or tenderness-within the tendon. This may occur anywhere along the tendon?s path, beginning with the tendon?s attachment directly above the heel upward to the region just below the calf muscle. Often pain appears upon arising in the morning or after periods of rest, then improves somewhat with motion but later worsens with increased activity. Tenderness, or sometimes intense pain, when the sides of the tendon are squeezed. There is less tenderness, however, when pressing directly on the back of the tendon. When the disorder progresses to degeneration, the tendon may become enlarged and may develop nodules in the area where the tissue is damaged.
Diagnosis
Examination of the achilles tendon is inspection for muscle atrophy, swelling, asymmetry, joint effusions and erythema. Atrophy is an important clue to the duration of the tendinopathy and it is often present with chronic conditions. Swelling, asymmetry and erythema in pathologic tendons are often observed in the examination. Joint effusions are uncommon with tendinopathy and suggest the possibility of intra-articular pathology. Range of motion testing, strength and flexibility are often limited on the side of the tendinopathy. Palpation tends to elicit well-localized tenderness that is similar in quality and location to the pain experienced during activity. Physical examinations of the Achilles tendon often reveals palpable nodules and thickening. Anatomic deformities, such as forefoot and heel varus and excessive pes planus or foot pronation, should receive special attention. These anatomic deformities are often associated with this problem. In case extra research is wanted, an echography is the first choice of examination when there is a suspicion of tendinosis. Imaging studies are not necessary to diagnose achilles tendonitis, but may be useful with differential diagnosis. Ultrasound is the imaging modality of first choice as it provides a clear indication of tendon width, changes of water content within the tendon and collagen integrity, as well as bursal swelling. MRI may be indicated if diagnosis is unclear or symptoms are atypical. MRI may show increased signal within the Achilles.
Nonsurgical Treatment
There is insufficient evidence from randomised controlled trials to determine which method of treatment is the most appropriate for the treatment of acute or chronic Achilles tendonitis. The patient should abstain from aggravating activities, but with a minimum of rest in order to preserve overall fitness. Possible treatments are non-steroidal anti-inflammatory drugs (NSAIDs), ice, rest, increased warm-up/stretching exercises, physiotherapy and heel lifts (orthotic devices - used on both sides to prevent a gait imbalance). Other treatments evaluated in a Cochrane review were heparin, steroid injections, glycosaminoglycan sulfate, Actovegin?, and topical laser treatment. There was no clear evidence of benefit from these. Casting is an option for resistant Achilles tendonitis. Drugs - analgesics and NSAIDs. Surgery is sometimes used for resistant Achilles tendonitis, but usually as a last resort. Other recently reported treatments include continuing sporting activity in conjunction with rehabilitation, low-energy shock wave therapy[4] and topical glyceryl trinitrate .
Surgical Treatment
Surgery is considered when non-operative measures fail. Patient compliance and postoperative management is an important aspect of the operative management to prevent ankle stiffness or recurrence of the symptoms. Surgery usually requires a removal of the damaged tissue (debridement) and meticulous repair of the tendon. Post-operative immobilization is required, followed by gradual range of motion and strengthening exercises start. It may require 6 months for the full recovery. Some known complication are recurrence, stiffness of the ankle and deep vein thrombosis.
Prevention
Regardless of whether the Achilles injury is insertional or non-insertional, a great method for lessening stress on the Achilles tendon is flexor digitorum longus exercises. This muscle, which originates along the back of the leg and attaches to the tips of the toes, lies deep to the Achilles. It works synergistically with the soleus muscle to decelerate the forward motion of the leg before the heel leaves the ground during propulsion. This significantly lessens strain on the Achilles tendon as it decelerates elongation of the tendon. Many foot surgeons are aware of the connection between flexor digitorum longus and the Achilles tendon-surgical lengthening of the Achilles (which is done to treat certain congenital problems) almost always results in developing hammer toes as flexor digitorum longus attempts to do the job of the recently lengthened tendon. Finally, avoid having cortisone injected into either the bursa or tendon-doing so weakens the tendon as it shifts production of collagen from type one to type three. In a recent study published in the Journal of Bone Joint Surgery(9), cortisone was shown to lower the stress necessary to rupture the Achilles tendon, and was particularly dangerous when done on both sides, as it produced a systemic effect that further weakened the tendon.
What Can Cause Pain At The Heel
Overview
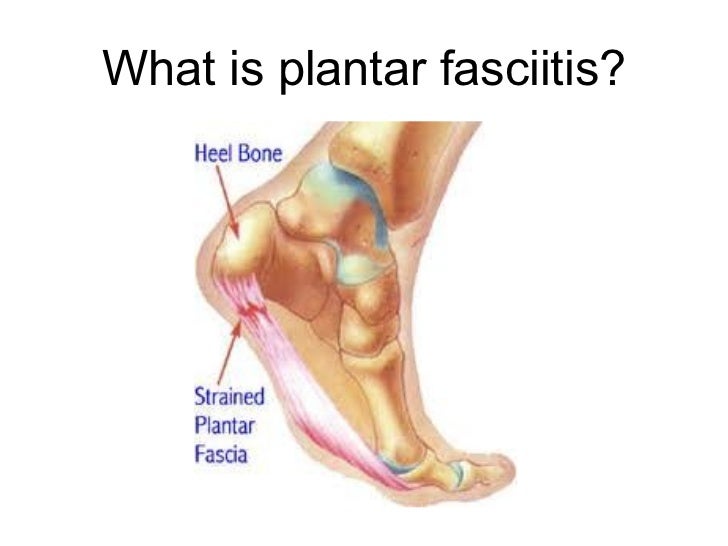
The plantar fascia is a thick, ligamentous connective tissue that runs from the heel bone to the ball of the foot. This strong and tight tissue helps maintain the arch of the foot. It is also one of the major transmitters of weight across the foot as you walk or run. Thus, tremendous stress is placed on the plantar fascia, often leading to plantar fasciitis- a stabbing or burning pain in the heel or arch of the foot. Plantar fasciitis is particularly common in runners. People who are overweight, women who are pregnant and those who wear shoes with inadequate support are also at a higher risk. Prolonged plantar fasciitis frequently leads to heel spurs, a hook of bone that can form on the heel bone. The heel spur itself is not thought to be the primary cause of pain, rather inflammation and irritation of the plantar fascia is the primary problem.
Causes
Plantar fasciitis most commonly occurs due to repetitive or prolonged activities placing strain on the plantar fascia. It is often seen in runners, or dancers and gymnasts who perform regular activities involving end of range foot and ankle movements. It may also occur in patients who walk excessively, especially up hills or on uneven surfaces. Older patients who spend a lot of time on their feet may also develop the condition. Plantar fasciitis frequently occurs in association with calf muscle tightness, inappropriate footwear, or biomechanical abnormalities, such as excessive pronation (flat feet) or supination (high arches). Occasionally the condition may occur suddenly due to a high force going through the plantar fascia beyond what it can withstand. This may be due to activities such as a sudden acceleration or a forceful jump.
Symptoms
Plantar fasciitis and heel spur pain usually begins in the bottom of the heel, and frequently radiates into the arch. At times, however, the pain may be felt only in the arch. The pain is most intense when first standing, after any period of rest. Most people with this problem experience their greatest pain in the morning, with the first few steps after sleeping. After several minutes of walking, the pain usually becomes less intense and may disappear completely, only to return later with prolonged walking or standing. If a nerve is irritated due to the swollen plantar fascia, this pain may radiate into the ankle. In the early stages of Plantar Fasciitis and Heel Spurs, the pain will usually subside quickly with getting off of the foot and resting. As the disease progresses, it may take longer periods of time for the pain to subside.
Diagnosis
Physical examination is the best way to determine if you have plantar fasciitis. Your doctor examines the affected area to determine if plantar fasciitis is the cause of your pain. The doctor may also examine you while you are sitting, standing, and walking. It is important to discuss your daily routine with your doctor. An occupation in which you stand for long periods of time may cause plantar fasciitis. An X-ray may reveal a heel spur. The actual heel spur is not painful. The presence of a heel spur suggests that the plantar fascia has been pulled and stretched excessively for a long period of time, sometimes months or years. If you have plantar fasciitis, you may or may not have a heel spur. Even if your plantar fasciitis becomes less bothersome, the heel spur will remain.
Non Surgical Treatment
Talk to your doctor about the best treatment plan for you. Options include. Apply ice or a cold pack to the heel and arch for 15 to 20 minutes several times a day. Wrap the ice or cold pack in a towel. Do not apply the ice directly to your skin. A special splint that will hold your foot in a neutral position while sleeping. Special shoe inserts that support the mid-arch region of your foot. Inserts that are not customized may work just as well as those that are customized. Activity. Avoid running and other activities that may worsen pain. Begin stretching exercises to lengthen the Achilles tendon and plantar fascia as recommended by your doctor. This is usually done when pain has lessened or improved. To help manage pain, your doctor may recommend over-the-counter nonsteroidal anti-inflammatory medication (NSAIDs), such as ibuprofen or naproxen. Prescription pain relievers may also be required. Steroid injections may be used in some cases or if other treatment is not working. A special type of sound wave called extracorporeal shock wave may also be considered in certain cases. This treatment happens under the care of your doctor. At this time, this is generally a treatment for long-term cases that do not respond to other treatments. Massage therapy or accupuncture may also be effective for long-term cases. In a few cases, basic treatments don't help. Surgery may be performed to cut the tight, swollen fascia.

Surgical Treatment
More invasive procedures to treat plantar fasciitis are usually sought only after other treatment has failed to produce favorable results. Corticosteroid injections deliver medicine into the injured fascia to reduce pain. However, this treatment may weaken the plantar fascia and result in further damage. In addition, extracorporeal shock wave therapy (ESWT) is a treatment where sound waves are sent through the damaged tissue in order to stimulate the damaged tissue and encourage healing. This method is relatively new in treating plantar fasciitis and your doctor will be able to tell you if it is the right method for you. Lastly, surgery is the last option for those suffering from chronic or severe plantar fasciitis.
Prevention
There are certain things that you can do to try to prevent plantar fasciitis, especially if you have had it before. These include regularly changing training shoes used for running or walking. Wearing shoes with good cushioning in the heels and good arch support. Losing weight if you are overweight. Regularly stretching the plantar fascia and Achilles tendon, especially before exercise. Avoiding exercising on hard surfaces.
What Brings About Heel Pain To Appear

Overview
If you experience sharp, throbbing or aching heel pain with your first steps out of bed each morning, or when walking throughout the day, you may be suffering from Plantar Fasciitis. This guide will help you to understand the definition, symptoms and causes of this condition and will explore your treatment options for rapid relief from your pain.
Causes
Plantar Fasciitis is caused by abnormal pronation of the foot. Contributing factors are obesity, weight gain, jobs that require a lot of walking or standing on hard surfaces, badly worn shoes with little support, and also inactivity. As a result of over-pronation, with every step the Plantar Fascia (band of tissue under the foot) is being stretched, resulting in inflammation, irritation and pain at the attachment of the fascia into the heel bone. In some cases the pain is felt under the foot, in the arch. Continuous pulling of the fascia at the heel bone, eventually may lead to the development of bony growth on the heel. This is called a heel spur. When you’re at rest, such as while sleeping, the Plantar Fascia tightens and shortens. When body weight is rapidly applied to the foot, the Fascia must stretch and quickly lengthen, causing micro-tears in the Fascia. As a result, the foot pain is more severe with your first steps in the morning, or after sitting for a long period. Plantar Fasciitis is more likely to happen if you suffer from over-pronation (flattening of the arch), you stand or walk on hard surfaces, for long periods, you are overweight or pregnant, you have tight calf muscles.
Symptoms
Plantar fasciosis is characterized by pain at the bottom of the heel with weight bearing, particularly when first arising in the morning; pain usually abates within 5 to 10 min, only to return later in the day. It is often worse when pushing off of the heel (the propulsive phase of gait) and after periods of rest. Acute, severe heel pain, especially with mild local puffiness, may indicate an acute fascial tear. Some patients describe burning or sticking pain along the plantar medial border of the foot when walking.
Diagnosis
The health care provider will perform a physical exam. This may show tenderness on the bottom of your foot, flat feet or high arches, mild foot swelling or redness, stiffness or tightness of the arch in the bottom of your foot. X-rays may be taken to rule out other problems.
Non Surgical Treatment
Your health care provider will often recommend these steps first Acetaminophen (Tylenol) or ibuprofen (Advil, Motrin) to reduce pain and inflammation. Heel and foot stretching exercises. Night splints to wear while sleeping to stretch the foot. Resting as much as possible for at least a week. Wearing shoes with good support and cushions. Other steps to relieve pain include aply ice to the painful area. Do this at least twice a day for 10 - 15 minutes, more often in the first couple of days. Try wearing a heel cup, felt pads in the heel area, or shoe inserts. Use night splints to stretch the injured fascia and allow it to heal. If these treatments do not work, your health care provider may recommend waring a boot cast, which looks like a ski boot, for 3 - 6 weeks. It can be removed for bathing. Custom-made shoe inserts (orthotics). Steroid shots or injections into the heel. Smetimes, foot surgery is needed.

Surgical Treatment
In unusual cases, surgical intervention is necessary for relief of pain. These should only be employed after non-surgical efforts have been used without relief. Generally, such surgical procedures may be completed on an outpatient basis in less than one hour, using local anesthesia or minimal sedation administrated by a trained anesthesiologist. In such cases, the surgeon may remove or release the injured and inflamed fascia, after a small incision is made in the heel. A surgical procedure may also be undertaken to remove bone spurs, sometimes as part of the same surgery addressing the damaged tissue. A cast may be used to immobilize the foot following surgery and crutches provided in order to allow greater mobility while keeping weight off the recovering foot during healing. After removal of the cast, several weeks of physical therapy can be used to speed recovery, reduce swelling and restore flexibility.
Stretching Exercises
Calf stretch. Lean forward against a wall with one knee straight and the heel on the ground. Place the other leg in front, with the knee bent. To stretch the calf muscles and the heel cord, push your hips toward the wall in a controlled fashion. Hold the position for 10 seconds and relax. Repeat this exercise 20 times for each foot. A strong pull in the calf should be felt during the stretch. Plantar fascia stretch. This stretch is performed in the seated position. Cross your affected foot over the knee of your other leg. Grasp the toes of your painful foot and slowly pull them toward you in a controlled fashion. If it is difficult to reach your foot, wrap a towel around your big toe to help pull your toes toward you. Place your other hand along the plantar fascia. The fascia should feel like a tight band along the bottom of your foot when stretched. Hold the stretch for 10 seconds. Repeat it 20 times for each foot. This exercise is best done in the morning before standing or walking.